

Common healthcare vulnerabilities in 2025 revealed less about any single weakness than about how complex, hybrid environments fail under real use. In Blaze Information Security’s 2025 pentest data, healthcare and pharmaceutical security assessments averaged 5.97 vulnerabilities per project against a 4.99 baseline across the overall pentest population, with 18.4% of findings rated High or Critical.
The sharper signal sits in the attack-vector distribution. Healthcare remains a network-driven sector, but it carries a higher share of local and physical vectors than the general pentest population, and a larger portion of findings that require some level of privilege, against a baseline where 53.0% of general findings require none.
The recurring weaknesses point to sensitive data exposure, inconsistent access control, and weak protection against authenticated abuse across patient-facing and internal systems. What follows is a closer look at where those failures concentrate and what the 2025 data reveals about how healthcare environments are actually built.
What Healthcare Penetration Tests Usually Cover
Penetration tests in the healthcare industry rarely focus on a single internet-facing application. Scope typically spans patient portals, supporting web applications and APIs, internal administrative platforms, and the on-prem and cloud infrastructure tied to clinical and operational workflows. In Blaze’s 2025 findings, healthcare and pharmaceutical assessments ran closer to this full-stack pattern than to the narrower, externally focused engagements common in SaaS or e-commerce.
That scope shapes the findings directly. A single assessment often has to evaluate several trust boundaries at once — patient access to electronic health records, clinician and staff workflows, privileged administrative functions, and system-to-system integrations with third-party vendors and business associates. Small identity or authorization failures at any one of those boundaries can expose patient data or break the role-based separation that frameworks like HIPAA depend on.
The impact profile reflects that reality. In the 2025 data, healthcare and pharmaceutical findings distribute more evenly across confidentiality, integrity, and availability than in most other sectors, which remain dominated by data exposure alone. That balance is a useful tell: a broken authorization check is serious, but so is a reliability issue in a system healthcare professionals depend on during a shift.
Severity and Finding Volume in Healthcare Pentests
Healthcare and pharmaceutical assessments averaged 5.97 vulnerabilities per project in Blaze Information Security’s 2025 data, placing the sector fourth out of eleven measured industries — behind Insurance (9.50), Oil, Gas & Energy (6.59), and Tech, Software & SaaS (6.34), and above the 4.99 baseline for the overall pentest population.
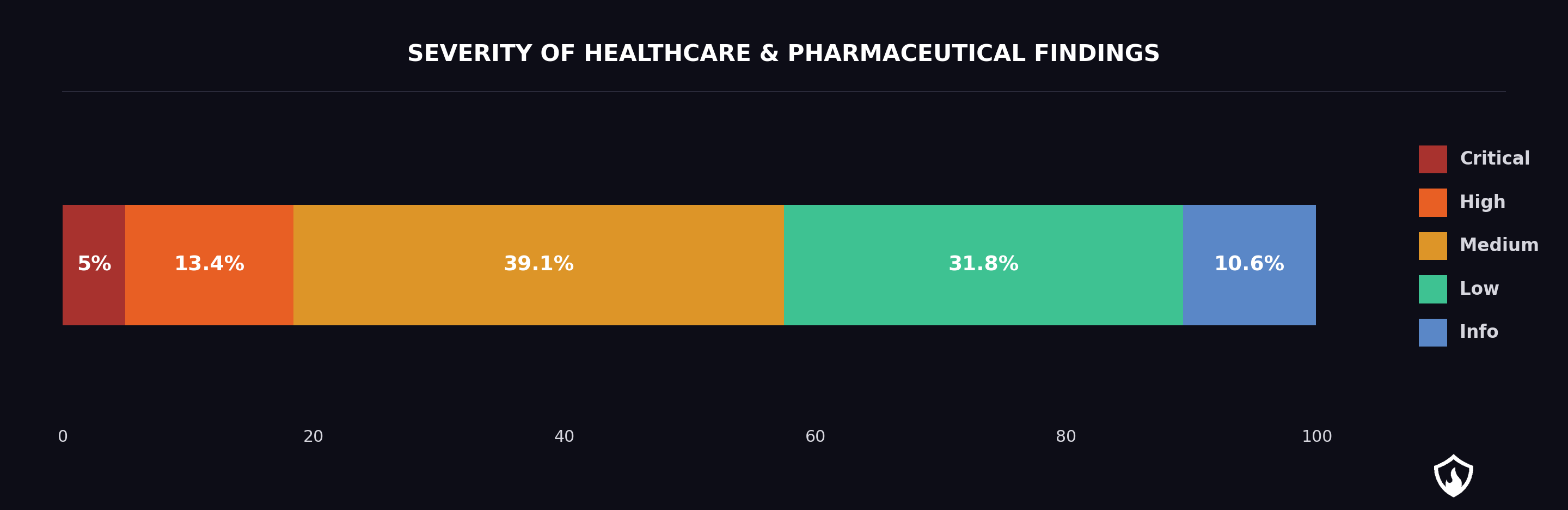
The severity profile tells a different story. 18.4% of healthcare findings were rated High or Critical, which places the sector mid-pack on severity concentration — above e-commerce, finance, transport, and telecoms, and below a cluster led by Education (32.0%), Public / Other Services (29.2%), and Insurance (27.6%). Healthcare does not rank as a severity hotspot. What it does show is a consistent pipeline of serious findings across a wider scope of systems than most other sectors cover.
A Medium finding in a patient portal login flow, a privileged administrative console, or an EHR integration endpoint can carry more practical risk than a High finding in a less-trafficked system: the exposure path is shorter, the data sensitivity is higher, and the blast radius extends into connected records and downstream systems.
Context from the wider threat landscape reinforces the point. Ransomware attacks have increased sharply in the healthcare sector, with attackers targeting hospitals due to their reliance on timely access to medical records, often demanding ransoms to restore access to critical systems. Healthcare organizations reported that over 67% faced ransomware attacks in 2025.
The same weaknesses pentests surface — authentication gaps, overexposed records, broken authorization — are the access points ransomware groups rely on to gain access and establish a foothold before encryption. Under that kind of pressure, even moderate-severity findings translate quickly into operational risk.
The Most Common Healthcare Pentest Findings
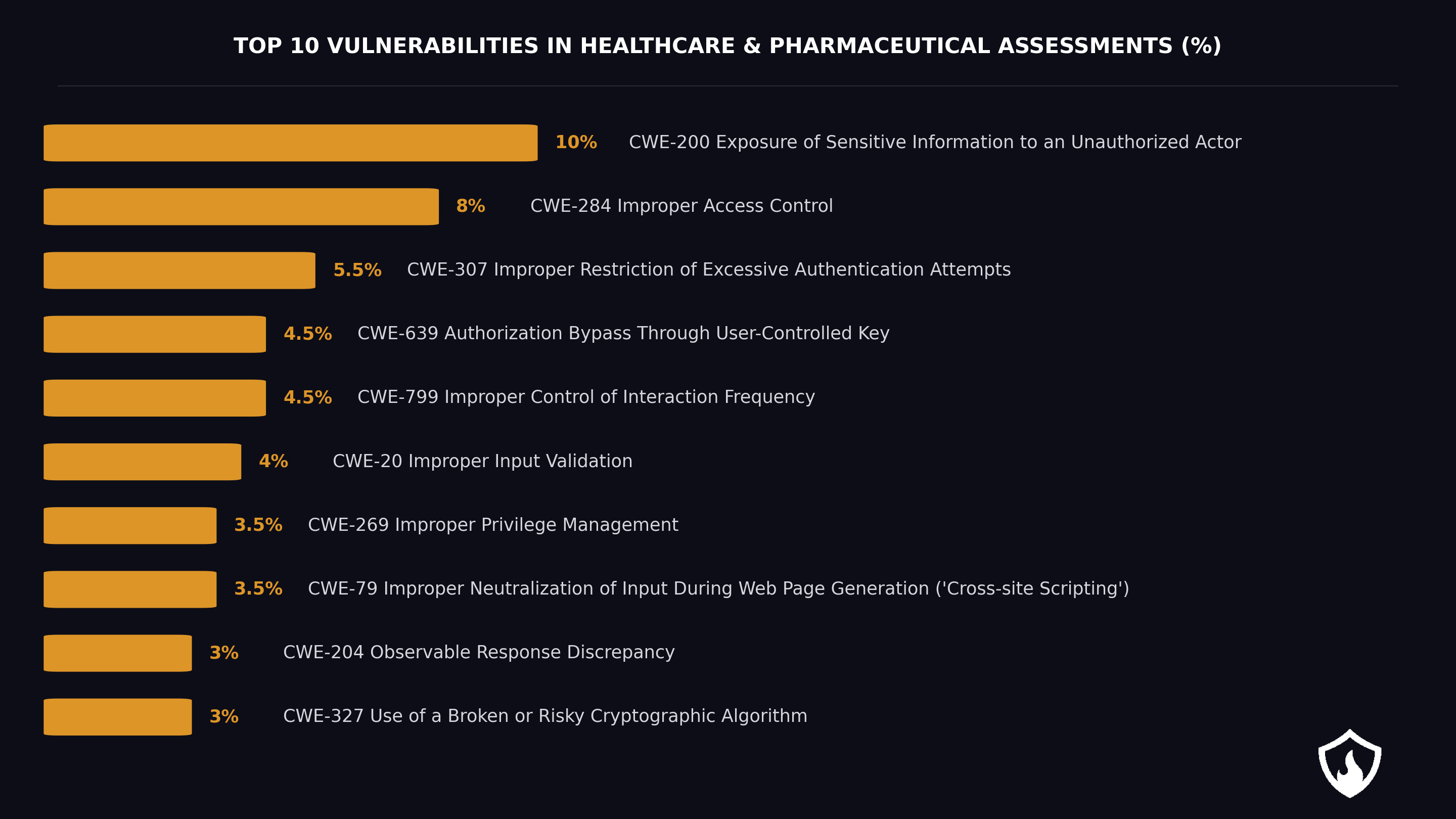
The top healthcare vulnerabilities point to a recurring pattern in this sector: too much information exposed, inconsistent control over who can reach which records or functions, and weak resistance to abuse once an attacker or low-privileged user starts interacting with the application. Out of 179 healthcare findings, the top five CWEs map directly onto these three failure modes.
CWE-200 (Exposure of Sensitive Information to an Unauthorized Actor) and CWE-284 (Improper Access Control) sit in the top three vulnerabilities across most sectors, including Finance & Fintech and Tech, Software & SaaS. The difference in healthcare is the third slot: CWE-307 (Improper Restriction of Excessive Authentication Attempts) ranks third here but falls outside the top three in most other industries, reinforcing how often authentication-abuse resistance lags in patient and clinician-facing systems.
For healthcare organizations and healthcare providers, that matters because these findings affect systems that process patient data, sensitive patient information, and other forms of healthcare data across patient-facing and internal workflows. CWE-200 surfaces in verbose API responses, error messages that leak identifiers, and searches over patient records that return more than the caller’s role should see. CWE-284 appears where role boundaries exist on paper but aren’t enforced across endpoints, background jobs, or admin tooling in healthcare systems.
What makes these vulnerabilities important is not just their frequency, but the kind of environments where they appear. In complex healthcare systems, small control failures can become unauthorized access, overexposure of sensitive healthcare data, or misuse of privileged functions. CWE-639 (Authorization Bypass Through User-Controlled Key) is the clearest example: a record identifier trusted from user input, letting a patient account at /records/12847 retrieve another patient’s medical records at /records/12846.
Rounding out the domain-relevant cluster is CWE-269 (Improper Privilege Management). Healthcare applications have to distinguish between patients, delegated family members, clinicians, administrative staff, and third-party integration users. When that distinction breaks down, privileged functionality, like record edits, access revocation, audit log manipulation, becomes reachable from accounts that should not touch it.
Primary Attack Vectors in Healthcare Penetration Testing
The way healthcare vulnerabilities are reached matters as much as the vulnerabilities themselves. In our engagements across all sectors, 85.1% of findings were network-reachable and 53.0% required no privileges to exploit, meaning an attacker with basic network access could act on more than half of them without authentication. Healthcare followed the same pattern, and in hybrid clinical environments that mix internet-facing portals, internal systems, and connected devices, “network-reachable” often translates to “reachable from a compromised workstation or a misconfigured segment.”
Web applications and APIs remain the most common entry point. Patient portals, scheduling tools, billing interfaces, and integration APIs concentrate access to Personal Health Information (PHI) in a small number of endpoints, which is why CWE-200, CWE-284 and CWE-639 (IDOR) dominate the healthcare findings. Authentication flaws such as CWE-307 amplify the risk because healthcare systems often keep legacy login flows alive for clinician convenience or vendor compatibility.
The spread of Internet of Medical Things (IoMT) equipment, such as infusion pumps, imaging systems, or monitoring hardware, has expanded the healthcare attack surface in ways that traditional pentests were not originally built to evaluate. Much of this hardware runs outdated software with limited patching pathways and minimal built-in security features.
Connected medical devices are often targeted due to their outdated software, which serves as a potential entry point for cybercriminals. The increasing number of Internet of Medical Things (IoMT) devices in healthcare has expanded the attack surface for cybercriminals, making medical equipment vulnerable to hacking due to outdated software and a lack of robust security features.
Social engineering and credential-driven attacks round out the picture. Phishing against clinical and administrative staff, credential stuffing against portals, and session-handling weaknesses (CWE-799, improper control of interaction frequency) give attackers a low-cost path into systems that are otherwise well-defended at the network layer. Combined with IoMT weaknesses and web-app flaws, these vectors explain why healthcare’s 5.97 average vulnerabilities per project understate the operational risk: the paths in are broad, and the assets behind them are sensitive.
What These Findings Mean
The recurring weaknesses healthcare pentest findings point first to PHI exposure and access control failure inside real workflows, not just to exposed perimeter services. The concentration of information exposure (CWE-200), improper access control (CWE-284), and IDOR (CWE-639) findings suggests that once an attacker reaches the application, too much sensitive healthcare data becomes reachable by unauthorized users through overly broad responses, weak role separation, or inconsistent enforcement of permissions.
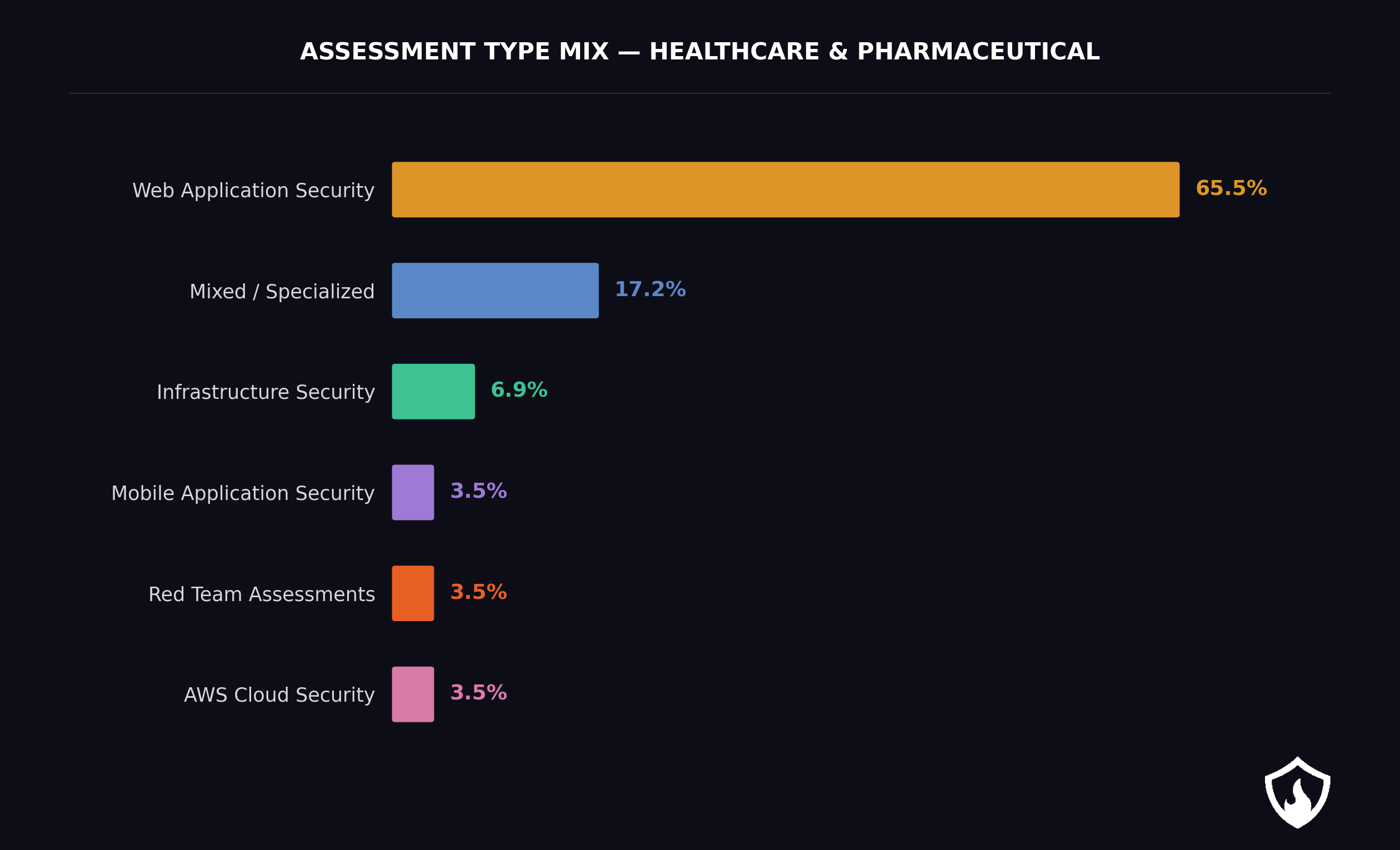
The findings also reflect the structure of the environment itself. Healthcare’s hybrid environments, like web systems, on-prem infrastructure, and specialized clinical applications, produce one of the largest mixed and specialized testing profiles in the industry breakdown. Every integration point creates another place for permissions and trust boundaries to drift out of alignment, which is why a single pentest scope often surfaces the same access control weakness in several places.
The deeper issue is identity and access in patient and staff workflows. A larger share of healthcare vulnerabilities requires some privileges to exploit, which means risk often emerges after initial access rather than only at the perimeter. For healthcare entities, that makes unauthorized access less about bypassing authentication entirely and more about what happens when permissions, trust boundaries, and application logic fail inside connected healthcare systems: the exact failure CWE-284 and CWE-639 describe.
All of this sits inside a regulatory environment that treats data protection as a statutory obligation, not a best practice. Healthcare organizations must comply with various regulations, including HIPAA, GDPR, and PIPEDA, which mandate strict data protection measures to protect sensitive patient data and can impose significant financial penalties for non-compliance. In 2024, the U.S. Department of Health and Human Services’ Office for Civil Rights (HHS OCR) issued USD $12.84 million in fines to healthcare providers for HIPAA violations related to healthcare data breaches.
How to Improve Healthcare Cybersecurity?
Addressing the vulnerability patterns above doesn’t require reinventing healthcare security: it requires applying a small number of controls consistently across the hybrid environments that generate these findings.
Implementing multi-factor authentication (MFA) adds an extra layer of security by requiring users to provide two or more forms of authentication before accessing sensitive healthcare data and systems. Applied to patient portals, clinician access, and vendor integrations, MFA directly counters the CWE-307 and credential-stuffing paths described earlier.
Regular employee training on cybersecurity awareness is crucial for educating staff on identifying and reporting potential cybersecurity threats, transforming employees from potential vulnerabilities into active participants in organizational defense. In healthcare, where phishing and social engineering remain primary attack vectors, training also covers the human side of access control — which requests to escalate permissions or share credentials should be refused.
Conducting regular security audits and vulnerability assessments helps identify and fix potential weaknesses in healthcare organizations’ systems, thereby enhancing their overall security posture. The 2025 data makes the case for continuous testing rather than annual check-ins: with 5.97 average vulnerabilities per project and 18.4% rated high or critical, a once-a-year scope rarely matches the rate at which healthcare systems change.
Zero Trust Architecture is recommended for healthcare cybersecurity, promoting the philosophy of “never trust, always verify” for all access points. That philosophy maps cleanly to the access control failures (CWE-284, CWE-639) driving the healthcare findings — it assumes the attacker is already inside the perimeter and forces each request to prove its legitimacy.
About This Data
All pentest findings were collected through VulnKeep, Blaze’s Penetration Testing as a Service (PTaaS) platform, and represent confirmed, validated vulnerabilities identified during live security assessments — not theoretical risks or automated scan results. To learn more about what 3294 vulnerabilities across different sectors reveal, download the full report.
Conclusion
Healthcare pentest findings in 2025 describe a sector where risk doesn’t come from a single dominant flaw but from the way hybrid environments fail under real use — at the points where patient portals, internal systems, and staff workflows meet. That is why manual penetration testing continues to matter in healthcare: it surfaces where protections exist on paper but break in practice.
The challenge ahead isn’t adding more controls — it’s making the ones already in place correct, consistent, and resilient where trust boundaries actually matter. Treated as ongoing risk management rather than a one-off compliance exercise, that approach keeps controls aligned with how healthcare environments actually evolve.
Frequently Asked Questions
What are the top healthcare vulnerabilities found in penetration tests?
In Blaze’s 2025 healthcare and pharmaceutical findings, the recurring pattern centers on PHI and other sensitive data exposure, weak access control and abuse-resistant authentication gaps, with the following top 5 vulnerabilities:
- CWE-200: Exposure of Sensitive Information to an Unauthorized Actor
- CWE-284: Improper Access Control
- CWE-307: Improper Restriction of Excessive Authentication Attempts
- CWE-639: Authorization Bypass Through User-Controlled Key
- CWE-799: Improper Control of Interaction Frequency
Because the main failures tend to happen inside trusted workflows, not only at the perimeter. Our report shows that healthcare environments combine patient-facing services, internal applications, and specialized systems, creating more opportunities for overexposed records, weak role separation, and post-login misuse of permissions.
What do healthcare penetration tests usually cover?
They usually cover more than a public web application. Healthcare and pharmaceutical environments are hybrid, combining web systems, on-prem infrastructure, and specialized internal applications.
How do healthcare pentest findings differ from general pentest findings?
General pentest results were heavily dominated by remotely exploitable, application-layer issues, with 85.1% of scored findings reachable over a network and 53.0% requiring no privileges. Healthcare still follows the application-driven pattern, but stands out for a higher presence of local and physical vectors, more findings that require some privileges, and a more balanced impact across confidentiality, integrity, and availability.
Why does the healthcare sector have such a broad attack surface?
Because healthcare systems rarely exist as one cleanly isolated platform. Blaze’s findings point to a sector shaped by patient portals, internal-facing systems, on-prem infrastructure, specialized applications, and integration-heavy workflows, which expands the number of trust boundaries and operational paths that a pentest has to evaluate.




